Resources
Guidelines for Burn Patient Referral
Developed to support clinical teams, these guidelines are intended to aid in referral decisions and should not be used as a substitute for professional judgment. If referencing or sharing these guidelines, please cite the American Burn Association as the original source.
If you have sustained a burn injury, please seek medical advice from a medical professional.
Find a Burn CenterDownload Guidelines
Advice on Transfer and Consultation
These guidelines are designed to support healthcare professionals in making informed clinical decisions regarding burn patient referrals. They are not definitive care recommendations but may help support the development of an effective local referral network.
Local and regional infrastructure, available resources, and existing provider relationships may influence when and where referral to a burn center is appropriate.
For individuals with burn injuries, these guidelines are not intended for self-assessment. Patients should consult a qualified healthcare provider for medical advice.
Burn Severity Determination
Superficial
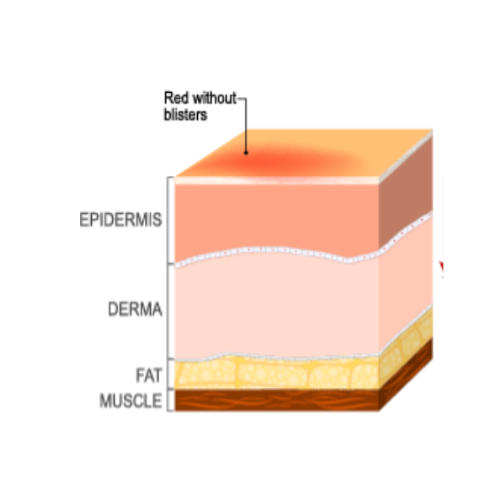
Superficial Partial Thickness
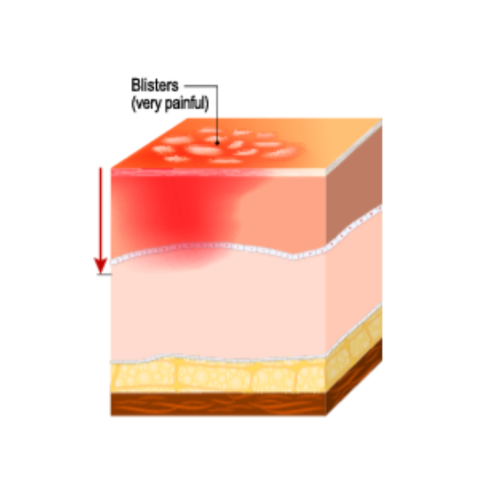
Deep Partial Thickness
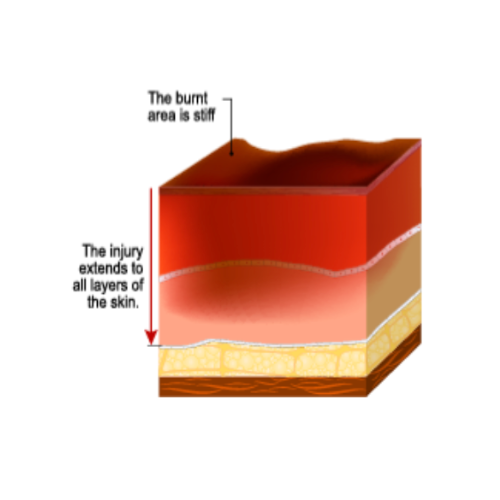
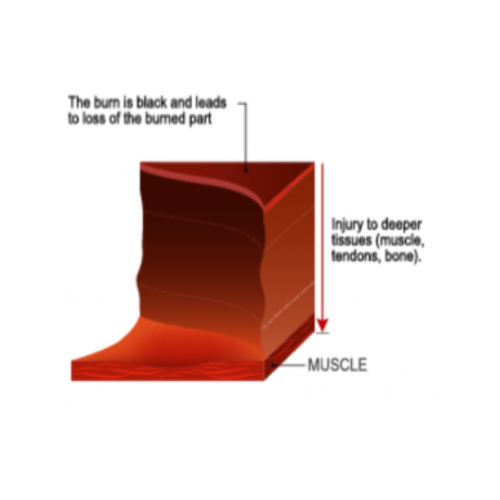
Full Thickness
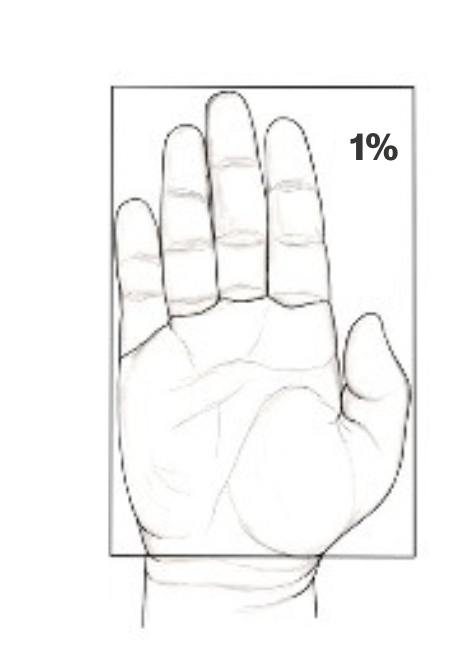
Percentage Total Body Surface Area (TBSA)
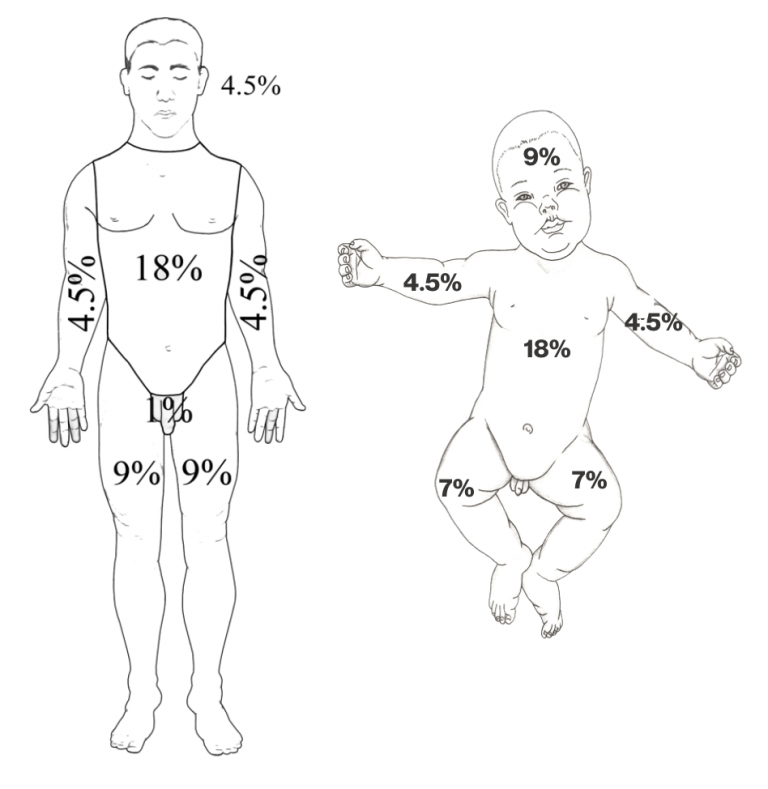
"Rule of Nines"